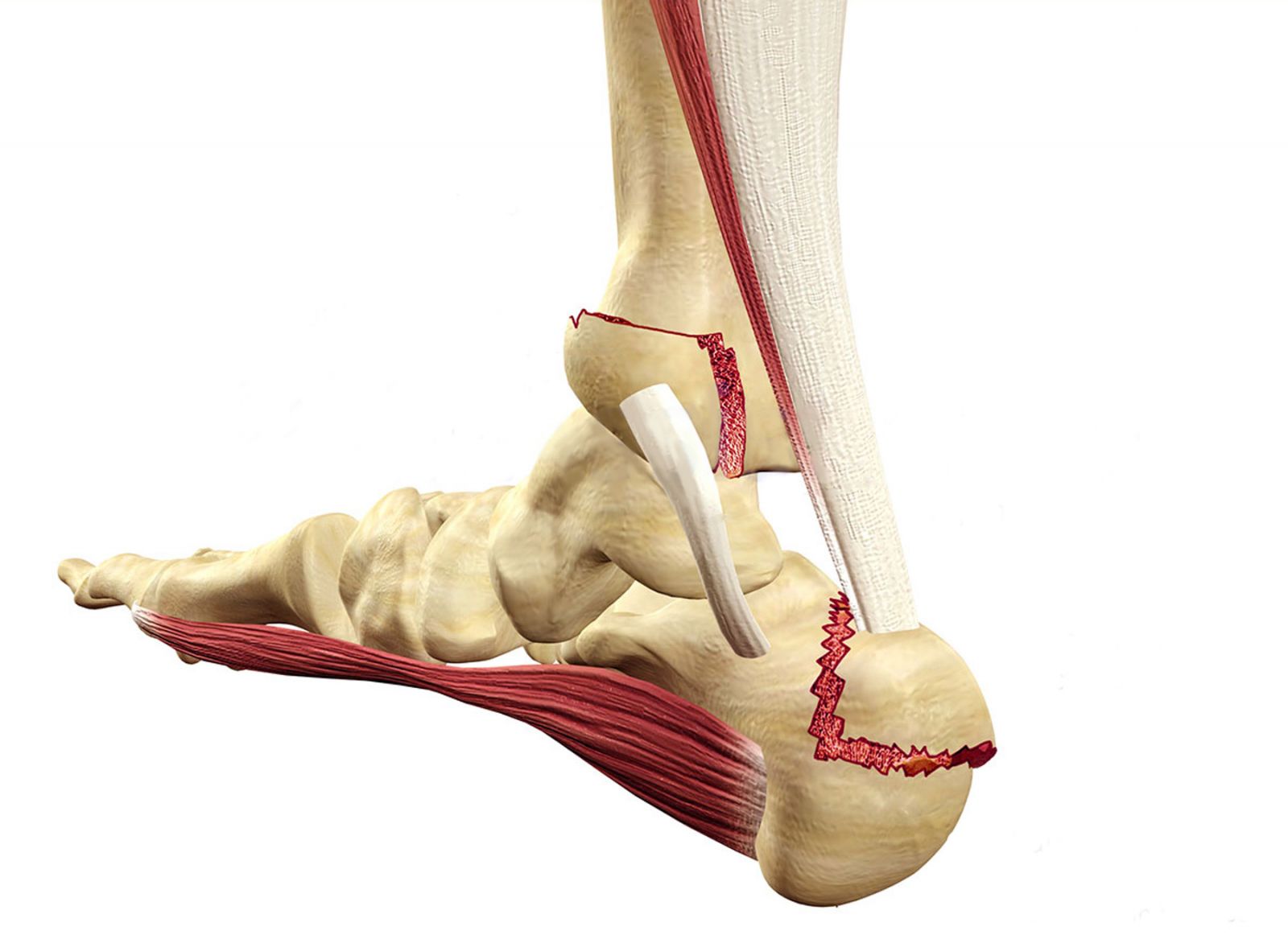
After trauma to the foot, a fracture may occur in any of the 26 bones. Depending on the location and severity of trauma, it is determined which bone is broken. In cases of falling from a height, the talus (knuckle bone) and calcaneus (heel bone) are mostly affected and may cause permanent problems for the patient. Fingers may be broken in direct impacts, and metacarpal bones may be broken in crushing injuries and sprains. In high-energy traumas, dislocations and fractures may accompany fractures, causing more pain and disrupting circulation.
Apart from fractures caused by trauma, stress fractures may arise from spontaneous foot pain in people who do heavy sports, soldiers, and sometimes women who stand a lot. Stress fractures are undissociated bone fractures that occur as a result of microtraumas without direct trauma.
Şikayet
Depending on the location and severity of the trauma, pain, swelling, bruising and deformed appearance may occur in the foot.
Muayene
In line with the information and complaints received from the patient, the foot structure is examined and swelling and bruises are evaluated. The area where the fracture is suspected is examined carefully, manually, without causing much pain to the patient. Due to the effect of foot fractures on circulation, the vessels and nail bed should be examined and the arterial and venous system of the foot should be seen to be normal.
Teşhis
The first option used for diagnosis is x-ray. Sometimes it may be necessary to request computerized tomography and magnetic resonance for fractures that are suspected or not clearly evident on x-ray. The scintigraphy method is diagnostic in stress fractures.
Tedavi
Early intervention should be done, followed up well, and the patient's foot should be elevated. Undissolved fractures and stress fractures are treated with a cast. Dissociated fractures can be wrapped in plaster after the installation procedure, or surgery may be required depending on the severity of the trauma. Correct and timely treatment is required to relieve foot pain and enable walking. While cast treatments generally vary between 4 and 6 weeks, longer treatment may be required for heel fractures. Although the complaints generally subside after the 3rd month, control is needed at every stage of the treatment. It is one of the treatment methods in which patient-doctor communication is at the forefront. Problems may not be resolved after plaster removal, patients may have trouble pressing immediately, osteoporosis may develop due to plaster treatment, and additional treatments may be needed.
